As a Registered Midwife, the chronic diseases that are relevant to my practice are: diabetes, chronic pain, and mental health. Mental health is the most commonly encountered chronic disease, with Major DepressiveDisorder (MDD) being the most observed. Depression is a relevant disease to my practice, as it has several implications for the parturient (pregnant person), and the child. Mental Health is also Chronic Disease of focus at the national and provincial level (Public Health Agency of Canada, Williams). For women taking medication for MDD, some will either change medications prior to becoming pregnant, in early pregnancy, or wean from their medication. Although there are safe medication options in pregnancy, many women feel stigma around taking antidepressants in pregnancy.

Supporting women to continue their medication as prescribes, adhere to the prescribers dosage adjustments, and engage in Cognitive Behavioural Therapy exercises (Haring) are roles Midwives fill for these pregnant patients. Our role is to also identify women who are developing MDD, and arrange consultation in a sensitive and timely manner. For some medications, particularly Selective Serotonin Reuptake Inhibitors (SSRIs), the neonate will have additional monitoring in their first day of life, as they complete their adaptation from fetal to neonatal circulation.
The rates of MDD in the perinatal population is comparable to that in the non-perinatal population at up to 16% (Williams) in British Columbia. Determinants of health that impact MDD include: Income and Social status, Social Supports and Coping Skills, Biology and Genetic Endowment, and Culture (Williams). Many of these determinants can factor into a pregnant person’s level of stress and ability to cope with life’s stresses.
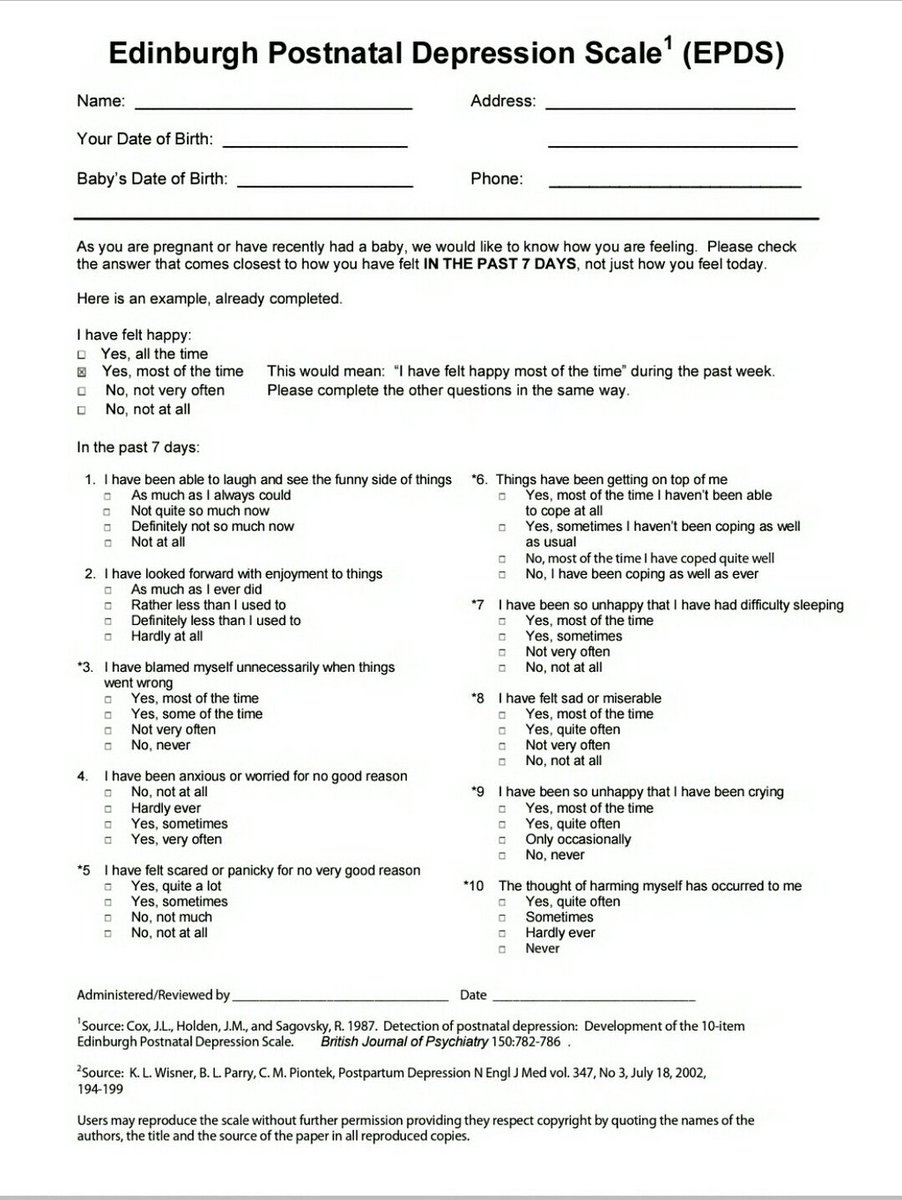
British Columbia has well developed guidelines and tools in place to support practitioners in caring for patients. These include Perinatal Services of BC’s Best Practice Guidelines for Mental Health Disorders in the Perinatal Period, Coping with depression during pregnancy and following the birth: A Cognitive-Behaviour Therapy-based self-management guide for women, and the standardized use of Edinburgh Prenatal/Postnatal Depression Scale (EPDS) (Williams, Haring). In my practice, I am grateful that I work in a model that provides continuity of care. This means that I work on a small team, getting to know our patients well throughout their childbearing year. I believe this is one of the greatest tools we have in supporting MDD as a chronic disease, and in prevention. However, one failure of our practice model is that our care ends at 6 weeks postpartum. This creates a transition for many women who may not feel comfortable talking with, or have easy access to, a family physician. Thankfully, Public Health helps to address this gap by performing routine phone check-ups with all postpartum moms around 8 weeks, which includes conducting an EPDS.
References
Williams, J. (2014, March). Best Practice Guidelines for Mental Health Disorders in the Perinatal Period (Canada, Perinatal Services of British Columbia). Retrieved from http://www.perinatalservicesbc.ca/Documents/Guidelines-Standards/Maternal/MentalHealthDisordersGuideline.pdf
Public Health Agency of Canada. (2015). Report from the Canadian chronic disease surveillance system: Mental illness in Canada, 2015. Retrieved from: http://healthycanadians.gc.ca/publications/diseases-conditions-maladies-affections/mental-illness-2015-maladies-mentales/alt/mental-illness-2015-maladies-mentales-eng.pdf
Haring, M. (2011, February). Coping with depression during pregnancy and following the birth: A Cognitive-Behaviour Therapy-based self-management guide for women. Retrieved https://reproductivementalhealth.ca/sites/default/files/uploads/resources/files/coping_with_depression.pdf